


The Problem with Clinician Fiefdoms, Alternative Care Models, and Transferring Memories via RNA Modification

“At some point, I switched to intellectual production from intellectual consumption.”
I stop stirring the spoon in my latte. I am at breakfast with Richard Ngo and we can finally hear each other; the barista has untwisted an audio cable, trading in shrill static for Turkish folk-rock. I later learn this genre is called Anatolian pop.
Richard is answering one of my favorite questions: “In Western civilization, there is a BC and an AD. What is the delineation between your personal BC and AD?” The change, he says, began during his master’s on the philosophy of machine learning which led to much of the writing on his blog. Richard’s comment strikes me because I think I am finally doing this. Writing about things that interest me, turning them into cocoon ideas instead of characters in a tweet. I’m still figuring out my voice (this is a source of discomfort because the more I narrativize my thoughts on healthcare and bio - and by extension, my thoughts on how to live - the more legible I become to people I don’t know).
Call it a commitment to full experimentation - not just in my writing but in how I live and work, and what I believe and produce. So thank you for bearing with my personal process and for listening just the same.
Purveyors of Non-Conventional Healthcare
I struggled with health this summer. Dull headaches crept in during afternoons, and I found myself waking up 3 or 4 times at night. The usual social and professional calendar no longer jived with an electrified New York (especially after a strange, isolated Covid-19 existence).
I consulted a gastroenterologist who recommended a health coach in Brooklyn. We’ll name her Sarah. I’ve worked happily with Sarah for almost 3 months now. I used to see her in person but now check-in over call and text due to my temporary domicile in Europe. We Facetime as I cook meals, notably a mushroom spinach tortellini paired with wine from 8greenbottles. I’m also in an opt-in group chat with some of Sarah’s other clients.
Studies show that behavioral interventions by non-clinicians can produce effective outcomes (see: sleep hygiene, physical therapy, nutrition). Individuals are increasingly turning to coaches, corresponding with the growth of advanced practice professionals like home health aides, doulas/midwives, and social workers.
This ties back to my previous post about the medical professional pipeline. To quickly summarize, constrained residency programs with diminishing federal subsidies have led to a physician shortage remedied by a convoluted web of technicians, administrators, and specialists. Psychiatry offers a textbook example: we already lack psychiatrists and psychiatry programs relative to patient demand. Yet additional clinical guidelines require specialization that choke the deficit further e.g. 5-6 years more training to become CAP (child and adolescent) certified.
Sure, there’s legitimate rationale for CAP-certification but bewildering compensation models are in overdrive. New specialties and sub-specialties spawn every year, with thousands now recognized by the American Medical Association. There’s an immunology physician for every major condition as well as obscure specialists like nocturnists (family medicine / internal medicine physicians who only work at night). Here’s a tiny sampling:

Our healthcare system can’t bear the cost and complexities of hyperspecialized clinical fiefdoms that rearrange - in perplexing ways - how individuals take action about their health. Patients are passed from clinician to specialist and back again. Care navigation this and outpatient that, proportionally complicated for underserved chronic patients. In response, people turn to alternative professionals that they understand like coaches.
Bessemer’s Morgan Cheatham shared his thoughts with me on community-led care as another example of non-conforming models:
Members of a community or people with a lived experience can provide invaluable stewardship, particularly within underserved communities. Queer women played an integral role in caring for folks during the HIV/AIDS epidemic. Black barbers are known for making impact #beyondthechair - sit in a barbershop and you’ll hear discussions on mental health to advice on diet/exercise. The traditional healthcare system doesn’t know how to value these interactions because they don’t fit neatly in the apparatus of medical billing and coding.
Startups are attempting to scale these alternative (consumer) care models. Folx for LGBTQ+ care. Livechair closing the “life expectancy gap of African Americans one barbershop at a time.” Chorus brings a community layer to therapeutic meditation. Papa for senior companionship.
Hospitals and doctors are claimants to technical competence but they sometimes obscure that medical care is artisanal. It’s a combination of science, technology, tradition, experience, learning, intuition. Healthcare only accounts for 10-20% of healthy population outcomes. Most docs agree:

We once relied on community and familial structures. Now we are reckoning with a medical establishment that has, perhaps unintentionally, neutralized decades of self-care as patients wade through forms and faxes and financing. Beyond public health initiatives, shifting support and education to navigators is at least a worthy complement to existing health services. A means of empowering individuals as capable stewards of their health.
What Does the Brain Have in Common with Snail Cannibalism?
After organ transplants, some patients claim personality changes and inexplicably pick up similar preferences/hobbies as their donors. “Inherited memories” are even pilfered for Hollywood: in romantic comedy Return to Me, Minnie Driver falls for David Duchovny after receiving his late wife’s heart.
The medical establishment has long written off inherited memories despite years of work by unorthodox psychologist James McConnell. In the 1960s at the University of Michigan, McConnell trained flatworms with flashlights and then ground up the masticated worms to feed new, untrained worms. The untrained cannibal worms appeared to exhibit the behavior of the trained ones, leading McConnell to propose the memory transfer hypothesis: outside of the brain’s central nervous system (especially the hippocampus, amygdala, and prefrontal cortex), might there be “memory RNA?”
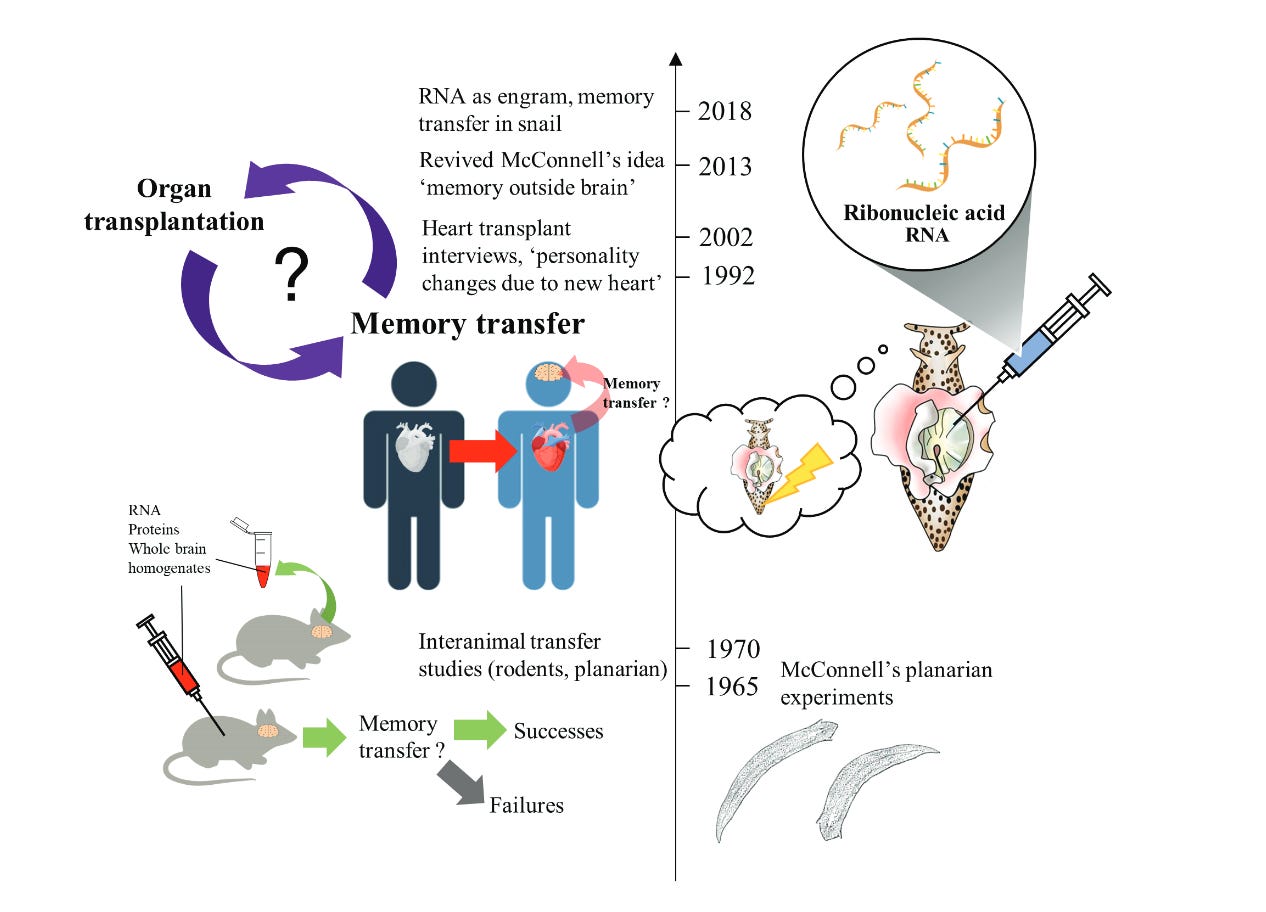
A research team at UCLA might have proven him right. At the very least, their results reignited the memory debate by transferring RNA between sea snails.

“Much to everyone’s surprise, the untrained snail recipients displayed defensive behaviour like their RNA-donor snail; even more fascinating is that this kind of defensive act is only replicated in the snails which received RNA from trained snails and not in those which received RNA from untrained snails.”
RNA is an inherent biological messaging system. If species are able to transfer memories genetically, it seems we know quite little about the biological basis for memory. Presents curious possibilities for gene therapy curing neurodegenerative diseases like Alzheimer’s…
Or stranger still, passing on memories to our friends and family.
Jobs and Hiring (From Friends of Waiting Room)
Nava Benefits is a benefits brokerage on a mission to bring high-quality affordable healthcare to every American. John is hiring for the business operations team
Cedar is a healthcare financial engagement platform that creates customized interactions for every patient. Dhruv / Jake are hiring a Director of Commercial Strategy and Go-to-Market
Fella helps men live longer and healthier lives, starting with an evidence-based program for clinical obesity. Luke is hiring a Head of Clinical Operations
Interesting Links and Tweets
More research on cellular barcoding. This nascent space will be huge for regenerative medicine, enabling investigation of cellular behavior in the body’s native environment. I’m tracking opinionated barcoding tools that help derive biological meaning from stem cell activity (e.g. tell me the regenerative differences between bone marrow cells after a blood cell transplant - and why it matters)
Language extinction triggers loss of unique medicinal knowledge
Niklas Rindtorff (physician-scientist at the German Cancer Research Center) and Arye Lipman (GP at MarsBio) offer ideas for a decentralized lab network:


Drugs finding second chances thanks to genetic data
A number of interesting Open Science projects have formed lately including SwartzDAO and French VC fund 2050 providing open-source models for their portfolio to accelerate market shifts in their industries
Lux’s Zavain Dar on an “Alphafold for the world’s biochemical structures,” linking to this Cassandra Quave piece on ethnobotany. Enveda and Hexagon Bio are two companies translating nature’s knowledge graphs for small molecule drug discovery:
After more than 20 years of research within Semma (acquired by Vertex for $950M), we now have the first patient ever cured of Type 1 diabetes. The NYT piece doesn’t expound on mechanisms involved - pancreatic stem cells harvested from a cadaver - and only cursorily mentions the participant was required to take immunosuppressants (not always an option for patients with numerous chronic and serious conditions). Still, I’m shaking with excitement if this spells the end of human suffering caused by T1
Sherman Leung on value-based vascular surgery. Note the paragraphs on supervised exercise therapy providing comparable durable improvement to (unnecessary) surgeries
Adam Fein’s commentary on CVS closing 900 pharmacies. Putting aside the San Francisco gab about theft, Fein notably points to low generic prices, CVS’s limited specialty dispensing, and competition from online pharmacies *ahem Truepill*
DynoTx engineer Stephen Malina muses about what’s (im)possible in synbio







----
Thank you to Morgan Cheatham, Kristin McDonald, Sahir Jaggi, and my sister for their comments.